





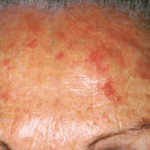
Actinic keratoses (solar keratoses)
11/08/2023
Alopecia areata
11/08/2023
Basal cell carcinoma (previously basal cell epithelioma) is the most common cancer for humans. There are an estimated 150,000 new cases each year in Italy, while in the United States, over 3.6 million cases are diagnosed annually. The number of basal cell carcinoma cases is increasing faster than any other tumor. It is a cancer that affects the skin and takes its name from the fact that the cells that degenerate are those located in the basal layer of the epidermis (the basal cells). Unlike other tumors, basal cell carcinoma has little or no tendency to spread by metastasis. Despite this, it is important to understand that it is in no way a benign tumor. In fact, it is difficult to eradicate in five to ten per cent of cases, and has a tendency to recur, as well as invading and destroying nearby tissues including muscles, cartilage and bone. As with most cancers, the early diagnosis and early treatment of basal cell carcinoma is the best weapon available.
> 1.000.000). E’ un processo tumorale che interessa la cute e prende il nome dal fatto che le cellule che degenerano sono quelle situate nello strato basale dell’epidermide quindi denominate Cellule Basali. Il Carcinoma Basocellulare o Epitelioma Basocellulare è anche il tumore umano con il più alto tasso di incremento per anno. A differenza di altri tumori, questo ha poca o nulla tendenza a diffondersi per metastasi; questo fatto non deve far pensare che si tratti di un tumore cosiddetto “benigno”. Infatti nel 5-10% dei casi è di difficile eradicazione, tende a recidivare e ad invadere e distruggere i tessuti vicini compreso i muscoli le cartilagini e l’osso.
Come per la maggioranza dei tumori anche per il Carcinoma Basocellulare o Epitelioma Basocellulare la diagnosi precoce ed il trattamento precoce è la miglior arma a disposizione della medicina.
Indice
Causes
In 90% of cases, basal cell carcinoma is caused by the excessive exposure to the sun or ultraviolet (UV) lamps.
Indeed, in nine out of ten cases, basal cell carcinoma appears on the areas of skin most exposed to UV light, such as the face, hairline for bald people, ears, shoulders, and back.
In the remaining 10% of cases, the causes of basal cell carcinoma are linked to genetics (familial form), or the use of drug treatments such as immunosuppressants (organ transplants), cortisone (chronic inflammatory or autoimmune diseases) or chemotherapy (neoplasms). X-ray treatments (radiotherapy, cobalt therapy) may also induce basal cell carcinoma.
People at risk
For cases of basal cell carcinoma caused by UV rays, individuals who are particularly at risk are those who:
- are sensitive to UV rays. This often applies to individuals with fair skin, blond hair, and blue eyes, or those with freckles and red/copper hair;
- engage in outdoor activities;
- spend or have spent long periods in tropical or equatorial areas, and
- use artificial tanning methods with UV rays
Warning signs
For early diagnosis and more effective treatment, it is important to know the warning signs of basal cell carcinoma.
These are:
- A lesion appears where the skin peels off and bleeds. Scabs form, which then peel off and reform again and again.

- An inflammatory plaque with no apparent cause appears and slowly expands

- A flesh-colored or reddened nodule forms

- A round erosion appears where the skin does not reform

- An area resembling a scar that was not caused by any trauma or injury appears

Dermatological assessment

caratteristiche del tumore. A dermatologist usually has no difficulty in diagnosing basal cell carcinoma from the clinical appearance alone.
In more difficult cases, a dermatologist may use a dermoscopic examination which uses a magnifying instrument on the lesion, the results of which can be assessed for the characteristics of the tumor.
In cases where the clinical and dermatoscopic diagnosis is critical, a histological examination is performed after taking a sample of the skin lesion under local anesthesia.

Clinical forms of basal cell carcinoma
There are many clinical forms of basal cell carcinoma.
Nodular form

A nodule appears that tends to slowly increase in size.
In the second stage, the nodule will ulcerate and bleed.
Confusion with moles
Many moles may be nodular, especially those on the face, and this can sometimes cause confusion with the nodular basal cell carcinoma.
However, the salient difference is that the mole will have been present for many years, unlike basal cell carcinoma nodules, which will have appeared recently.
Miescher’s nevus (MN) of the face

Nodular basal cell carcinoma

Ulcerated basal cell carcinoma next to a nevus of Miescher

Basal cell carcinoma: treatment options
Although a rarely metastasizing and therefore relatively benign tumor, basal cell carcinoma has a surprising ability to reappear after treatment. One reason for this behavior is that basal cell carcinoma does not have defined margins, and nests of tumor cells can be found even at some distance from the identified tumor core. Another reason is that the skin where the basal cell carcinoma tumor appears is already sufficiently damaged to reproduce another one, either in the immediate or distant future. The earlier a basal cell carcinoma tumor is identified and the earlier action is taken, the higher the chances of therapeutic success.
Surgery
Surgery is still the standard treatment of choice today.
It is performed under local anesthesia and removes the tumor with a portion of apparently healthy tissue around it.
However, the downsides of surgery are the often high cost, likelihood of tumor recurrence and evident scarring which may cause aesthetic discomfort.
Thermal destruction
Basal cell carcinoma can be destroyed by either hot or cold thermal waves that are generated through treatment techniques such as radiofrequency, laser therapy or liquid nitrogen, etc.
However, thermal destruction has many drawbacks such as scarring, damage to healthy tissue, possibility of infection of the treated area, and the recurrence of the tumor.
For these reasons, thermal destruction has been replaced by more viable techniques.
Mechanical destruction
Basal cell carcinoma can also be removed mechanically with a sharp spoon (curette) that enucleates the tumor tissue from healthy tissue.
Mechanical destruction or curettage has drawbacks such as scarring and the possibility of the tumor recurring.
Destruction with x-rays (ionizing rays)
Destruction of basal cell carcinoma with X-rays, although possible, has now been abandoned because of the danger of inducing ray damage to healthy boundary cells, which could trigger the emergence of a new radio-induced tumor.
Treatment with topical pharmaceuticals
Photodynamic therapy (PDT): protocols for basal cell carcinoma
The protocol for ALA-PDT treatment of basal cell carcinoma involves many variations depending on tumor type, site, skin type, duration of injury, etc. The most common variations are the time of exposure to ALA and the number of PDT sessions to be scheduled.
- Examination, photographic documentation, additional investigations
- Patient information valid for obtaining informed consent
- Preparation of the lesion for PDT when necessary
- Application of 10% ALA with a suitable applicator
- Occlusion of the treated part with polyethylene film (or similar) to enhance penetration of the product
- Covering the treated area to prevent light penetration
- Waiting for development of protoporphyrin IX from between two to four hours, as indicated
- After the determined time has elapsed, removal of the dressing
- Observation of fluorescence with wood lamp as an index of protoporphyrin IX development
- Exposure of the ALA-treated area to red light for the amount of time it takes for the fluorescence to disappear (in the range of ten minutes, varying according to the light source)
- Upon completion, dressing of the treated area with PEG Ointment and cotton gauze
- At home, continuation of dressing with PEG Ointment once daily for a week
- After 30 days, if requested by the dermatologist, a second PDT session in the same manner as above may be performed
- Clinical follow-ups can be scheduled for three, six and/or twelve months after
- In case of tumor recurrence, new PDT sessions can be scheduled or another treatment route can be investigated
Results in the treatment of basal cell carcinoma with ALA-PDT
According to data from international studies, the success rate from treating basal cell carcinoma with ALA-PDT matches that which can be obtained with traditional surgery, and surpasses that which can be obtained with destructive methods (laser therapy, cryotherapy, radiofrequency, etc.). The strengths of ALA-PDT treatment are:
- No scarring and better cosmetic result
- No anesthetic
- No damage to healthy tissue surrounding the lesion
- Able to treat multiple lesions at the same time
- Able to treat extensive lesions or those not suitable for surgery
- Suitable for individuals who have not been cleared for surgery
For these reasons, ALA-PDT treatment is considered as a therapy for basal cell carcinoma and should be offered to patients with this type of skin cancer.
Treatment with topical pharmaceuticals
The drug 5-fluorouracil (5-FU) is a chemotherapeutic that blocks cell reduplication and has been used in creams to treat basal cell carcinoma. However, the drug’s poor manageability and frequent tumor recurrences have limited its use.
The drug imiquimod (an immunomodulator) in cream has also been used to treat these tumors but skin irritation, long healing time, frequent recurrences, and high cost have limited its use.
Examples of PDT treatment





{kind=link}
{kind=link}
{kind=link}